"Nurse allocation" wasn't a single problem. It was three problems that had to be solved in sequence, by different users, at different times of day.
Evening / Morning before
Who is seeing which patient, and when?
Nurse Manager / Charge Nurse
See each nurse's caseload for the coming day. If a nurse calls out, redistribute that caseload across the remaining team — quickly, without losing track of who's covered.
Before run
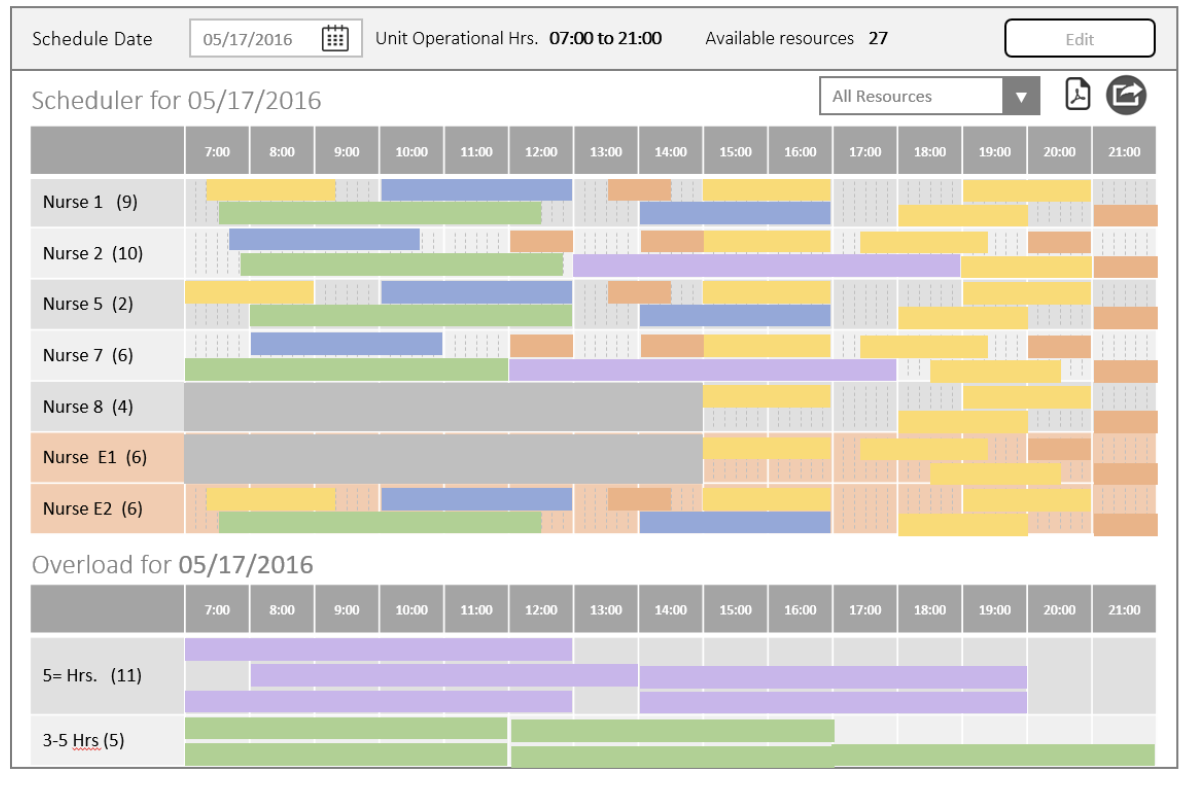
What happens when there aren't enough nurses?
Nurse Manager / Charge Nurse
When scheduled patients outnumber available nurses, the system needs to surface the gap clearly — not hide it. The manager needs to see exactly what's unallocated and make manual decisions to cover it.
Throughout day
Patient arrives — which nurse takes them?
Flow Coordinator / Charge Nurse
As patients check in — including same-day add-ons — a flow coordinator needs to direct each patient to their assigned nurse in real time, without hunting through a list or making phone calls.
Design challenge
The architecture had to support three distinct user states: planning mode the night before, adjustment mode the morning of, and reactive mode throughout the day — without the interface feeling schizophrenic. Every constraint here had a patient safety implication.